This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputsThis e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
Hyndavi Konakanchi, Intern
7/1/23
A CASE DISCUSSION OF 60/M ON ACUTE CVA (HAEMORRHAGIC) WITH RIGHT SIDED HEMIPLEGIA K/C/O HTN ON IRREGULAR MEDICATION
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Following is the view of my case :
A 60 yr old gentle man came to casuality with CHEIF COMPLAINTS of difficulty in walking, inability to speek and unable to move Right hand and Right leg since 19/1/23 night
HISTORY OF PRESENT ILLNESS :
Pt was apparently normal until 1 yr back then he had fever for which he went to RMP and diagnosed to have hypertension ,but used medication only on giddiness episode (ie.., not on regular medication)
Now on; 19/1/23 night , the whole problem started at 1 am in the night when he woke up from sleep and woke her wife up telling that he wants to urinate but he couldn’t get up from the bed ; then her wife brought a bottle to empty his urine inspite of this he couldn’t pass the urine in bottle , he passed all over the bed and floor
After 30 mins he again woke her wife up again telling he wants to urinate,but couldn’t get up and again she brought the bottle to empty but he passed all over the bed and floor, but this time there is a new complaint of slurring of speech
On 20/1/23 morning at 6 am he woke up and walked with a stick to washroom to pass stools , after passing stools he walked to house with his son’s support then seeing the patients condition attenders called local RMP to their home, he checked his BP and found to have 170 systolic bp and then he gave some medication ? Nitroglycerin , after that as the patient’s condition didn’t improve , they got frightened and then they decided to take the patient to some hospital , they started at their home at 1 pm as they live in boyyagudem, thirumalagiri sagar ( mandal ) , Nalgonda district it took 3 hrs to reach to our hospital.
By 4 pm on 20/1/23 they came to our hospital
PAST HISTORY:
30 yrs back he had abdominal pain and diagnosed to have appendicitis, for which he underwent appendicectomy
25 yrs back , while he was at farm in the day time, suddenly he had he fell down , he had paralysis of right leg , for which pt was taken to Kurnool , there at some hospital they gave some medications and then they had their cultural beliefs and stayed for some days in temple and did Pooja for his recovery , after that they returned to their home , pt couldn’t walk and he took rest for about 4 months and then he started walking with support of stick , finally when pt thought he could walk without support he back to farm
3 yrs back , he had h/o RTA and sustained shaft of femur fracture, for which surgery was done and there is implant inserted
OCCUAPATIONAL HISTORY:
He was farmer from his 20 yrs of age ( 40 yrs back ) , after that from his 40 yrs ( 20 yrs back ) he is working as a security guard in Hyderabad till his recent fracture incident , from then he is not doing any work.
DAILY ROUTINE:
When he was farmer , he used to wake up at 5am in the morning and freshen up & eat rice and curry, by 8 am he used to go farm with the lunch box and does his usual works in the farm &eats his dinner at 12pm in the farm itself , he returns to home by 6pm , then freshen up — haves his dinner by 8pm and drinks Natu Sara ( an alocoholic drink available mainly in villages , which is now banned by govt ) daily
When he was security guard his routine is dependent on the shift he has ie., 1 week there he had morning 8am - 8pm ; then he wakes up at 6am in the morning — freshen up — eats curry and rice — goes to work place by 8 am with lunch box — does his duty & eats his lunch by 12 pm — he returns to home at 8 pm , then freshen up — haves his dinner by 8 pm and drinks 2-3 quarter daily
After his femur fracture, he was completely at home , as he stopped working; he wakes up at 7 am in the morning he freshens up and takes care of their cattle ( in their home ), eats curry rice — watches TV — eats lunch by 12 pm — sleeps for a while — goes to market & he spends some time talking with his neighbours — comes to home — eats dinner by 8 pm — drinks ~alternative days ( 2-3 times per week ) — goes to sleep by 10 pm
ALCOHOLIC HISTORY:
He started taking alcohol from 40 yrs ( when his age is 20 yrs ) initially he used to take daily Natu Sara as mentioned above , then he started taking quarter daily after Sara has been banned .He mostly prefers drinking alone on regular days & with their relatives on festivals , functions, family gatherings
But after the fracture incident he stopped drinking daily but he drinks 2/3 times a week
SMOKING HISTORY:
He started smoking BIDI 1 pack/ day since 40 yrs ( when his age is 20 yrs ) and he continues to smoke till date ; he didn’t decrease smoking after his accident; in this way it is different from the alcohol history
MEDICAL HISTORY:
* He is K/c/o HTN and is on irregular medication from 1 yr
Not a K/C/O asthma / Ischemic heart disease / epilepsy / TB / DM
FAMILY HISTORY
No significant family history
PERSONAL HISTORY
OCCUPATION : retired security guard
DIET : Mixed
APPETITE : Normal
SLEEP : Normal
BOWEL AND BLADDER HABITS : Normal
ADDICTIONS: alcohol (90/180ml per day) and bidi addiction (1 pack - 20 per day )
GENERAL EXAMINATION
* Patient is concious
* Built - moderately built , moderately nourished
VITALS
Blood pressure : 180/100 mm hg
Pulse Rate : 51 bpm
RR : 17cpm
Temperature : 98.7 degrees F
SPO2 : 91% under 8L of O2
GCS : E4V1M1
* NO PALLOR,ICTERUS , CYANOSIS, CLUBBING , LYMPHADENOPATHY ,EDEMA






SYSTEMIC EXAMINATION
RESPIRATORY SYSTEM :
Inspection : bilateral symmetrical chestPalpation: trachea centrally placed, bilateral symmetrical chest movements
Percussion: resonance
Auscultation: Bilateral air entry is present , NVBS , no adventitious sounds heard
PER ABDOMEN :
Inspection: obese
Palpation :soft non tender
Auscultation: bowel sounds heard
Percussion: resonant note
CVS:
S1 S2 heard, JVP not rised
CNS:
speech absent
RT LT
Tone : UL N N
LL N N
Power : UL 0/5 5/5
LL 5/5 5/5
MSE : not elicitable
Reflexs :
B T S K A P
Rt ++. Extensor
Lt Absent Extensor
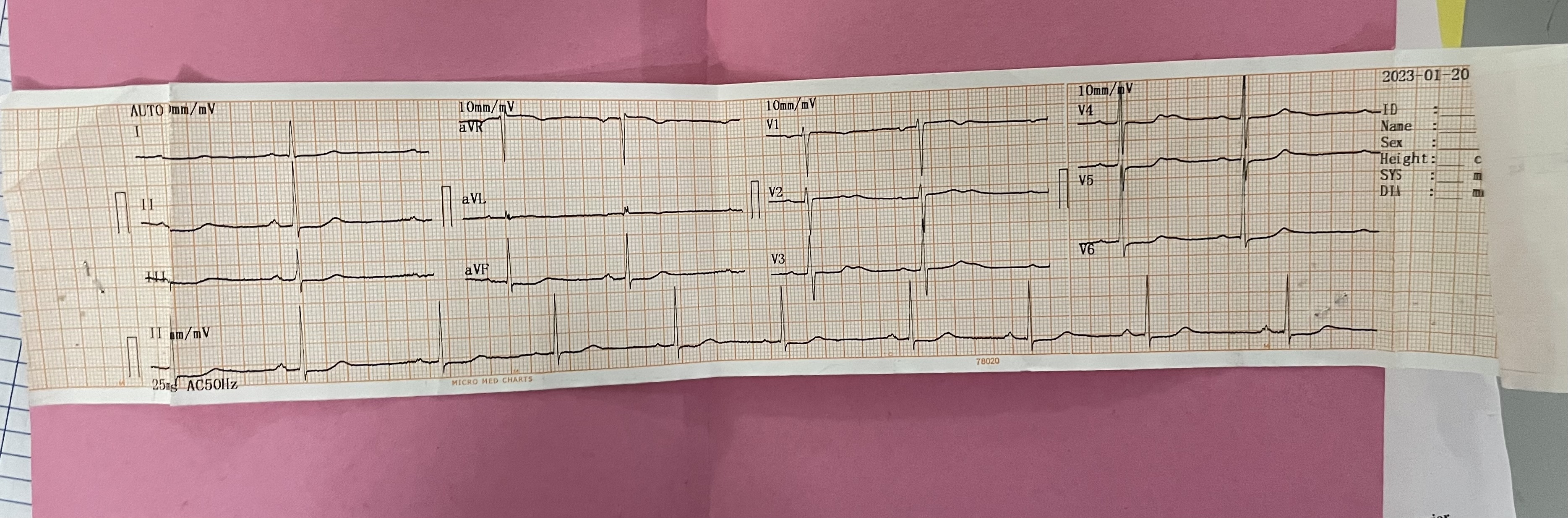
INVESTIGATIONS:
On 20/1/23
On 22/1/23
On 23/1/23
On 24/1/23
MRI IMAGES
CT BRAIN VIDEO LINK :
DIAGNOSIS :
ACUTE CVA (HEAMORRHAGIC) WITH RIGHT SIDED HEMIPLEGIA K/C/O HTN ON IRREGULAR MEDICATION
TREATMENT :
IVF NS @ 100 ml/hr
Tab.paracetamol 650 mg po/sos
Inj.Leviteracetam 500 mg in 100 ml Ns Iv
Inj.Mannitol over 10-15 mins tid
Tab.Nicardia retard 10 mg tid
Inj. Optineuron Iv/od
Bp monitoring and GCS monitoring hrly
Monitor vitals & temp charting and inform sos
Physiotherapy for both upper and lower limbs
Inj.pitaz 4.5 g tid
Hrly oral suction
SOAP NOTES :
21/01/2023
UNIT 5
DR HIMAJA, PGY1
DR PAVANI, PGY2
DR SAICHARAN, PGY3
DR ABHINAYA, SR
DR HYNDAVI, INTERN
DR AKASH, INTERN
ICU DAY 1
AGE : 60 GENDER :M
S:
stools not passed since yesterday
no fever spikes
no sleep , no appetite
no headache
O:
pt conscious, coherent, co-operative
Bp-170/100 mm hg
PR-60 bpm
Grbs-134 mg/dl
I/o - 1400/700
Temp-98°F
CVS - S1,S2 heard , no added sounds
RS - BAE + , NVBS
PA - Soft,Non tender
CNS- speech absent
RT LT
Tone : UL N N
LL N N
Power : UL 0/5 5/5
LL 5/5 5/5
MSE : not elicitable
Reflexs :
B T S K A P
Rt ++. Extensor
Lt Absent Extensor
A:
Acute CVA - Heamorrhagic presented with HTN Emergency with Right sided Hemiplegia k/c/o HTN SINCE 1 yr on irregular medication
P:
IVF NS @ 100 ml/hr
Tab.paracetamol 650 mg po/sos
Inj.Leviteracetam 500 mg in 100 ml Ns Iv
Inj.Mannitol over 10-15 mins tid
Tab.Nicardia retard 10 mg tid
Tab.Vitamin B1 10mg RT/OD
Vitamin B2 10mg
vitamin B3 45mg
vitamin B5 50mg
vitamin B6- 3mg
B12- 15mcg
Bp monitoring and GCS monitoring hrly
monitor vitals
22/01/2023
UNIT 5
DR HIMAJA, PGY1
DR PAVANI, PGY2
DR SAICHARAN, PGY3
DR ABHINAYA, SR
DR HYNDAVI, INTERN
DR AKASH, INTERN
ICU DAY 2
AGE : 60 GENDER :M
S:
stools not passed since yesterday
no fever spikes
no sleep , no appetite
no headache
O:
pt conscious, coherent, co-operative
Bp-160/90 mm hg
PR-76 bpm
Grbs-125 mg/dl
I/o - 2900 / 1650
Temp-98.3 F
CVS - S1,S2 heard , no added sounds
RS - BAE + , NVBS
PA - Soft,Non tender
CNS- speech absent
RT LT
Tone : UL N N
LL N N
Power : UL 0/5 5/5
LL 5/5 5/5
MSE : not elicitable
Reflexs :
B T S K A P
Rt ++. Extensor
Lt Absent Extensor
A:
Acute CVA - Hemorrhagic presented with HTN emergency; Right sided Hemiplegia k/c/o HTN SINCE 1 yr on irregular medication
P:
IVF NS @ 100 ml/hr
Tab.paracetamol 650 mg po/sos
Inj.Leviteracetam 500 mg in 100 ml Ns Iv
Inj.Mannitol over 10-15 mins tid
Tab.Nicardia retard 10 mg tid
Inj. Optineuron Iv/od
Bp monitoring and GCS
monitoring hrly
monitor vitals & temp charting and inform sos
Physiotherapy for both upper and lower limbs
Inj.pitaz 4.5 g tid
Hrly oral suction
23/01/2023
UNIT 5
DR HIMAJA, PGY1
DR PAVANI, PGY2
DR SAICHARAN, PGY3
DR ABHINAYA, SR
DR HYNDAVI, INTERN
DR AKASH, INTERN
ICU DAY 3
AGE : 60 GENDER :M
S:
stools not passed since 3 days , flatus passed
fever spikes +
no sleep , no appetite
no headache
O: pt is not conscious/coherent/cooperative
Bp-140/90 mm hg
PR-70 bpm
Grbs-105 mg/dl
I/o - 2500 / 950 ml
Temp-98.9 F
CVS - S1,S2 heard , no added sounds
RS - BAE + , grunting +
PA - Soft,Non tender
CNS- GCS: E not elicitable V1M1
speech absent
RT LT
Tone : UL N N
LL N N
Power : UL 0/5 5/5
LL 5/5 5/5
MSE : not elicitable
Reflexs :
B T S K A P
Rt ++. Extensor
Lt Absent Extensor
A:
Acute CVA - Heamorrhagic presented with HTN emergency ; Right sided Hemiplegia k/c/o HTN SINCE 1 yr on irregular medication
P:
IVF NS @ 100 ml/hr
Tab.paracetamol 650 mg po/sos
Inj.Leviteracetam 500 mg in 100 ml Ns Iv
Inj.Mannitol over 10-15 mins tid
Tab.Nicardia retard 10 mg tid
Inj. Optineuron Iv/od
Bp monitoring and GCS
monitoring hrly
monitor vitals & temp charting and inform sos
Inj.pitaz 4.5 g tid
Hrly oral suction
25/1/23
UNIT 5
DR HIMAJA, PGY1
DR PAVANI, PGY2
DR SAICHARAN, PGY3
DR ABHINAYA, SR
DR HYNDAVI, INTERN
DR AKASH, INTERN
ICU DAY 4
AGE : 60 GENDER :M
S:
stools not passed since 5 days
no fever spikes
no sleep , no appetite
no headache
O: pt is not conscious
Bp-160/110 mm hg
PR-74 bpm
Grbs-118 mg/dl
I/o - 2700/2100 ml
Temp-98.6 F
CVS - S1,S2 heard , no added sounds
RS - decreased breath sounds
P/A - Soft,Non tender
CNS- GCS: E4V1M1
speech absent
RT LT
Tone : UL N N
LL N N
Power : UL 0/5 3/5
LL 0/5 3/5
MSE : not elicitable
Reflexs :
B T S K A P
Rt ++. Extensor
Lt Absent Extensor
A:
Acute CVA - Haemorrhagic presented with HTN Emergency ; Right sided Hemiplegia k/c/o HTN SINCE 1 yr on irregular medication
P:
IVF NS @ 100 ml/hr
Tab.paracetamol 650 mg po/sos
Tab.Clinidipine 10 mg Rt/Bd
Inj.Leviteracetam 500 mg in 100 ml Ns Iv
Inj.Mannitol over 10-15 mins tid
Tab.Nicardia retard 10 mg tid
Inj. Optineuron Iv/od
Bp monitoring and GCS
monitoring hrly
monitor vitals & temp charting and inform sos
Inj.pitaz 4.5 g tid
Hrly oral suction
Proctolytic enema
25/01/2023
UNIT 5
DR HIMAJA, PGY1
DR PAVANI, PGY2
DR SAICHARAN, PGY3
DR ABHINAYA, SR
DR HYNDAVI, INTERN
DR AKASH, INTERN
ICU DAY 5
AGE : 60 GENDER :M
S:
stools not passed
Cough +
No fever spikes
no headache
O: pt is not conscious
Bp-160/100 mm hg
PR-69 bpm
Grbs-178 mg/dl
I/o - 2600/1300 ml
CVS - S1,S2 heard , no added sounds
RS - decreased breath sounds
P/A - Soft,Non tender
CNS- GCS: E4V1M6
speech absent
RT LT
Tone : UL increased increased
LL increased increased
Power : UL 0/5 4/5
LL 0/5 4/5
Reflexs :
B T S K A P
Rt ++. Extensor
Lt Absent Extensor
A:
Acute CVA - Hemorrhagic in lt superior parietal lobe and right thalamus presented with HTN Emergency ; Right sided Hemiplegia k/c/o HTN SINCE 1 yr on irregular medication
P:
IVF NS @ 100 ml/hr
Tab.paracetamol 650 mg po/sos
Tab.Clinidipine 10 mg Rt/Bd
Inj.Leviteracetam 500 mg in 100 ml Ns Iv
Inj.Mannitol over 10-15 mins tid
Tab.Nicardia retard 10 mg tid
Inj. Optineuron Iv/od
Bp monitoring and GCS
monitoring hrly
monitor vitals & temp charting and inform sos
Inj.pitaz 4.5 g tid
Hrly oral suction
Hrly position change
26/01/2023
UNIT 5
DR HIMAJA, PGY1
DR PAVANI, PGY2
DR SAICHARAN, PGY3
DR ABHINAYA, SR
DR HYNDAVI, INTERN
DR AKASH, INTERN
ICU DAY 6
AGE : 60 GENDER :M
S:
stools passed
no fever spikes
no headache
O: pt is not conscious
Bp-170/100 mm hg
PR-74 bpm
Grbs-102 mg/dl
I/o - 2600/1300 ml
CVS - S1,S2 heard , no added sounds
RS - diffuse crepts
P/A - Soft,Non tender
CNS- GCS: E4V1M6
speech absent
RT LT
Tone : UL increased increased
LL increased increased
Power : UL 0/5 4/5
LL 0/5 4/5
Reflexs :
B T S K A P
Rt ++. Extensor
Lt Absent Extensor
A:
Acute CVA - Hemorrhagic in lt superior parietal lobe and right thalamus presented with HTN Emergency ; Right sided Hemiplegia k/c/o HTN SINCE 1 yr on irregular medication
P:
IVF NS @ 100 ml/hr
Tab.paracetamol 650 mg po/sos
Tab.Clinidipine 10 mg Rt/Bd
Tab.Telma H Rt/Od
Inj.Leviteracetam 500 mg in 100 ml Ns Iv
Inj.Mannitol over 10-15 mins tid
Tab.Nicardia retard 10 mg tid
Inj. Optineuron Iv/od
Bp monitoring and GCS
monitoring hrly
monitor vitals & temp charting and inform sos
Inj.pitaz 4.5 g tid
Hrly oral suction
Hrly position change
































Comments
Post a Comment