A 33 YEAR OLD MAN WITH PANCREATITIS, PSEUDOCYST AND LEFT BRONCHO-PLEURAL FISTULA
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputsThis e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
Hyndavi Konakanchi, 8th semester
Roll no: 63
May 13, 2021
A CASE DISCUSSION ON PANCREATITIS, PSEUDOCYST AND LEFT BRONCHO PLEURAL FISTULA
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Following is the view of my case :
(All this information was given by patient relative to Dr. K.Vaishnavi PG 2 )
CASE PRESENTATION:
* A 33 yr old male daily wage labourer from miryalaguda who is a chronic alcoholic and smoker came to hospital on 30/04/2021 with CHEIF COMPLAINTS of pain abdomen & vomiting since 1 week and constipation, burning micturition, fever since 4 days.
HISTORY OF PRESENT ILLNESS:
* Patient was apparently asymptomatic 5 yrs back when he had painabdomen & vomitings for which he was taken to a local hospital and treated conservatively.
* Following that he stopped taking alcohol as advised by the physician and was symptom free for nearly 3 yrs.
* Later he again started taking alcohol following which he had recurrent episodes of pain abdomen & vomiting
* (5-6 episodes in the past 1 year) which were treated by a local RMP.
* From the past 20 days he had increased amount alcohol consumption (5 bottles of toddy per day)
* Last binge of alcohol 1 week back following which he again had pain abdomen & vomiting from 1 week and fever from 4 days.
* abdominal pain in umbilical, left hypochondriac, left lumbar and hypogastric regions.
* Abdominal pain was incresed after food intake.
* Pain is throbbing type and radiating to back and is associated with nausea and vomiting( 1 episode) , which is non bilious, non projectile and also has food particles and water content 1 week.
* Fever was high grade, continuous and associated with chills and rigors.
* Not associated with loose stools.
* Then he developed constipation since 4 days and passing flatus.
* patient also had burning micturition since 4 days, which is associated with suprapubic pain, increased frequency and urgency
* No history of blood or mucus in stools.
* No other complaints.
PAST HISTORY:
* No history of hypertension, diabetes mellitus, tuberculosis.
* No history of previous blood transfusions or any surgeries.
PERSONAL HISTORY:
* Appetite: decreased
* Diet: mixed
* Bowel and bladder movements: ## Constipation
## Has burning micturition since 4 days
* Additions:1) Consumed 3 sara bottles per day for 5 yrs and then stopped for 3 yrs and again started drinking from last 1 yr which increased to 5 bottles per day from past 20 days.
2) khaini : 1 per day since 5 yrs.
3) Ghutka: 5 per day since 6 months.
FAMILY HISTORY:
Not significant
GENERAL EXAMINATION:
Patient is conscious coherent and cooperative.
He is well oriented to time, place and person.
He is thinly built and moderately nourished.
VITALS:
Temperature: Afebrile
Pulse Rate: 90 beats per minute
Blood pressure: 110/70 mm of Hg
Respiratory Rate: 22 cycles per minute
SpO2: 95% on room air
No Pallor
No Icterus
No Cyanosis
No Clubbing
No Lymphadenopathy
No Edema
( Vitals measured by Dr. K.Vaishnavi PG 2 )
SYSTEMIC EXAMINATION:
1) Abdominal examination:


Inspection:
Shape of the abdomen: distended
Umbilicus: everted
* No visible pulsations
* All quadrants of abdomen are moving equally on respiration.
* Grey turner sign ( bluish discolouration of flanks) and Cullens sign( bluish discolouration of periumbilical area ) are negative [ These are +ve in patients with severe pancreatitis with Haemorrhage ]
Palaption:
* No local rise of temperature
* Tenderness present over umbilical, left hypochondriac, left lumbar, hypogastric and suprapubic region.
* Guarding and rigidity : present
* No palpable masses found
* Liver and spleen are not palpable
Percussion :
* Liver span: normal
Ascultation:
* Sluggish bowel sounds are heard.
2) Respiratory system:
* Intially Resp system : Decreased air entry and Fine inspiraory crackles noted in left isa ,iaa ma ,inter scapular areas and normal on right side
* Later pt developed progressive pneumothorax - Absent air entry on left side all areas
* No wheeze.
*Position of trachea : central
3) CVS:
* S1 and S2 heart sounds are heard
*No murmurs
4) CNS:
* No abnormality detected
( Examination done by Dr. K.Vaishnavi PG 2 )
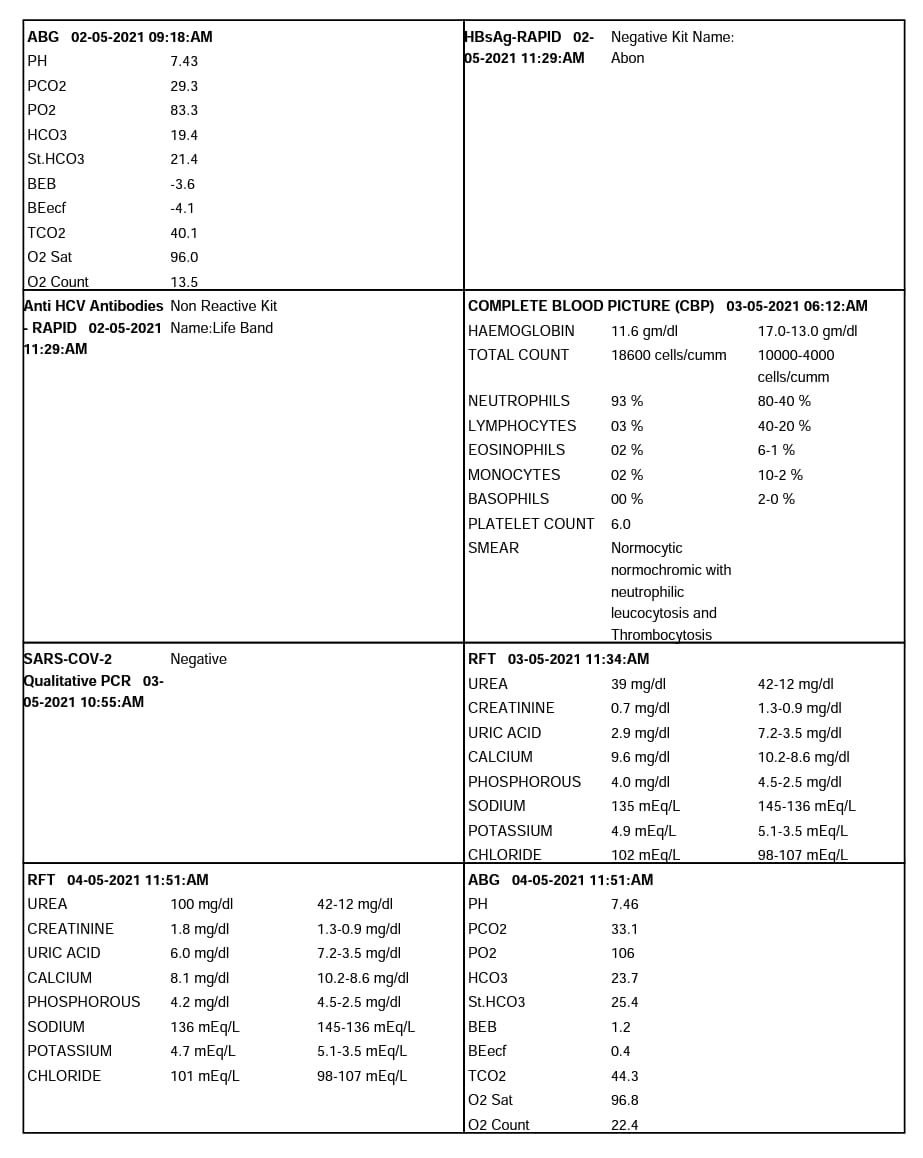
INVESTIGATIONS:
* CBP( Complete Blood Picture ), LFT( Liver Function tests ), RFT( Renal Function Test ) , Urine analysis, Serum amylase, ABG( Areterial Blood Gas ), Pleural tapping.
( Pictures below are taken by Dr.Vamshi PG 1)




* Imaging:
( pictures mentioned below are taken by Dr. K.Vaishnavi PG 2 )
1) CE CT ( Contrast Enhanced CT):
* Showing pseudocyst and infective fluid collections



2) Chest x ray:
* 1 st image showing pleural effusion and basal atelectasis and 2 nd image shows pneumothorax ( collapsed lung ) which developed in the course of hospital.

* CBP showed LEUCOCYTOSIS.
* LFT showed Increased ALP and decreased ALBUMIN.
* Pleural fluid was EXUDATIVE in nature according to lights criteria and pleural fluid amylase being: 469 mg/dl.
* CE CT abdomen shows ; LARGE PSEUDOCYST COMPRESSING STOMACH (Dimensions: 15*9*10 cms ) & MULTIPLE INFECTIVE FLUID COLLECTION IN MIDLINE ALONG ANTERIOR ABDOMINAL WALL AND SUB HEPATIC REGION; WHICH ARE CONTINUOUS AND LOCULATED ASCITIS.
* Chest x ray showed; MODERATE PLEURAL EFFUSION , BASAL ATELECTASIS IN LEFT LUNG
LEFT PNEUMOTHORAX SECONDARY TO BRONCHO PULMONARY FISTULA
DIAGNOSIS:
* ACUTE ON CHRONIC PANCREATITIS WITH PSEUDOCYST & ACUTE INFECTIVE PERI PANCREATIC FLUID COLLECTIONS
* MODERATE LEFT PLEURAL EFFUSION WITH BASAL ATELECTASIS.
* LEFT PNEUMOTHORAX SECONDARY TO BRONCHO PLEURAL FISTULA
* BISAP SCORE — 2 points out of 5 ( SIRS, PE )
{ B- Blood urea nitrogen, I- Impaired mental status, S- SIRS (Systemic Inflammatory Response Syndrome), A- Age, P- Pleural effusion }
TREATMENT & COURSE IN HOSPITAL:
* Patient was initially treated with;
1) ING. MEROPENAM ; TID for 7 days
2) ING. METROGYL 500 mg IV TID for 5 days
3) ING. AMIKACIN 500 mg IV BD for 5days
4) TPN ( Total Parenteral Nutrition )
5) IV NS / RL at the rate 12l ml per hour
6) ING. OCTREOTIDE 100 mg SC , BD
7) ING. PANTOP 40 mg IV , OD
8) ING. THIAMINE 100 mg in 100 ml NS IV , TID
9) ING. TRAMADOL in 100 ml NS IV , OD
## But inspite of this therapy for 4 days , patient has constant fever spikes and rised TLC and patient was deteriorating clinically, with tachypnoea , Acute kidney disease and SVT ( Sinus tachycardia ) with increased abdominal distension and guarding.


The information below has been borrowed by me from various sources that I have referenced and acknowledged with their online links and I have paraphrased them further,also request my readers to visit their original site as it was very useful to me
https://www.ncbi.nlm.nih.gov/books/NBK482468/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5849938/
https://surgery.ucsf.edu/conditions--procedures/pancreatic-pseudocysts.aspx#mobile_menu
Davidson's principles and practice of medicine textbook
CASE DISCUSSION:
* The cause of pancreatitis here may be attributed to alcohol.
* In acute pancreatitis; there is premature activation of zymogen granules in pancreas leading to increased release of proteases into surrounding tissues.
* Acute pancreatitis is often self limiting condition but in some patients with severe disease or frequent recurrent episodes of acute pancreatitis; like in this case is associated with complications like pseudocyst formation, necrosis etc.., And also systemic complications.
* Following an inflammatory rupture of pancreatic duct, a collection of fluid & debris may develop in lesser sac known as pancreatic fluid collection
* Initially it has poorly developed fragile granulation tussue wall which after 6 weeks developed into a fibrous capsule and forms PSEUDOCYST!
* CE CT is a confirmatory test here and most important in diagnosis as it will also show the local complications and other supportive investigations like : CBP , LFT, serum amylase , pleural fluid analysis ....
* And also a persistent rise of level of serum amylase can suggest pseudocyst cyst formation ( like in this case)
* The diagnosis of :
ACUTE ON CHRONIC PANCREATITIS WITH PSEUDOCYST & ACUTE INFECTIVE PERI PANCREATIC FLUID COLLECTIONS
* MODERATE LEFT PLEURAL EFFUSION WITH BASAL ATELECTASIS.
* LEFT PNEUMOTHORAX SECONDARY TO BRONCHO PLEURAL FISTULA
Was made!
TREATMENT ALONG WITH RATIONALE:
1) ING. MEROPENAM ; TID for 7 days
* Meropenem ( broad spectrum Carbepenem ) an antibiotic.
2) ING. METROGYL 500 mg IV TID for 5 days
* inj. Metrogyl has METRONIDAZOLE
( Nitroimidazole drug ) an antibiotic
3) ING. AMIKACIN 500 mg IV BD for 5days
* It is an Aminoglycoside antibiotic
## Here all three of these (Inj. Meropenem, Inj. Metrogyl, Inj. Amikacin ) are used as antibiotics to control infection and ; to prevent septic complications of acute pancreatitis.
4) TPN ( Total Parenteral Nutrition )
* Method of feeding that by passes gastrointestinal tract
* Fluids are given to vein , it provides most of the nutrients body needs.
* TPN has proteins, carbohydrates, fats, vitamins, minerals.
5) IV NS / RL at the rate 12l ml per hour
* Given for fluid replacement ie., treat dehydration
6) ING. OCTREOTIDE 100 mg SC , BD
* It is a Somatostatin long acting analogue.
* It is used here to decrease exocrine secretion of pancreas and it also has anti- inflammatory & cytoprotective effects.
7) ING. PANTOP 40 mg IV , OD
* Inj. Pantop has PANTOPRAZOLE ( Proton Pump Inhibitor) used for its anti pancreatic secretory effect.
8) ING. THIAMINE 100 mg in 100 ml NS IV , TID
* It is B1 supplement.
* It is given here because; due to long fasting & TPN usage , body may develop B1 deficiency
* Wernicke encephalopathy secondary to B1 deficiency may be caused... so a prophylactic B1 supplemention is necessary.
9) ING. TRAMADOL in 100 ml NS IV , OD
* It is an opioid analgesic, given to releive pain
## After 4 days of this treatment; there is no improvement in patient and infact he is deteriorating clinically !!!
* So USG GUIDED MALECOT DRAIN - PLACED INSIDE AND PSEUDOCYST WAS DRAINED
* TWO OTHER USG GUIDED DRAINS ARE PLACED TO DRAIN THE PERI-PANCREATIC COLLECTIONS
## After this patient was dramatically improved but in the mean time he developed PNEUMOTHORAX IN LEFT LUNG !!!
* Oxygen supply for mild hypoxia
* And ICD ( Inter Coastal Drain ) was placed.


Comments
Post a Comment